
Being a medical professional like a pharmacist, physical therapist or social worker, you need to learn a unique thought process by facilitating uncomplicated yet accessible long-term retention. One way to achieve this is through the application of a clinical SOAP in your work. SOAP significantly meets the challenge of providing efficiency while sustaining quality. If you are currently learning your way in the medical field , this article will be helpful for you in writing the clinical SOAP note or progress note of the patients. So, we include some clinical SOAP note templates to guide you in your healthcare or social service work. Keep on reading!
FREE 9+ Clinical SOAP Note Samples
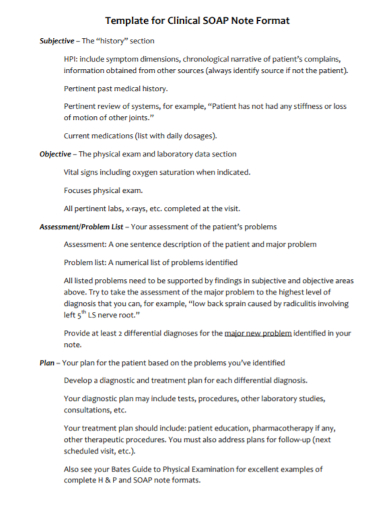
1. Clinical SOAP Note
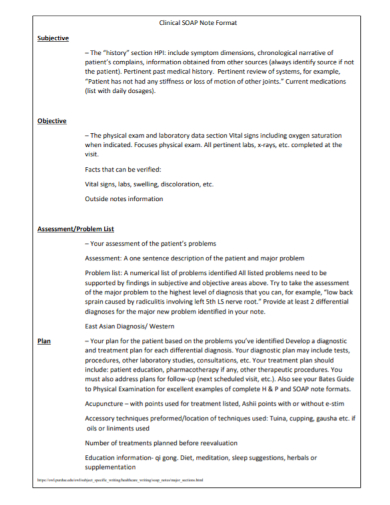
2. Clinical SOAP Note Format
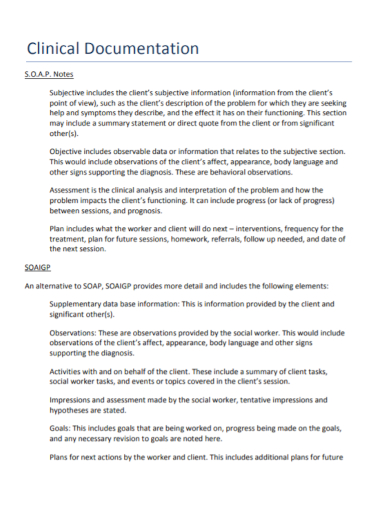
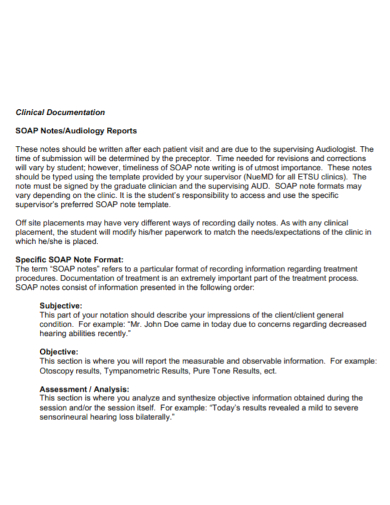
3. Clinical Documentation SOAP Note
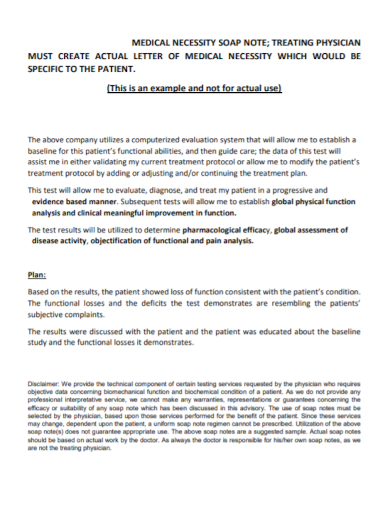
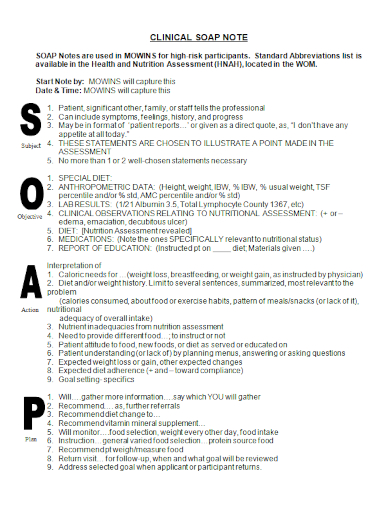
4. Medical Necessity Clinical SOAP Note
5. Clinical SOAP Case Note

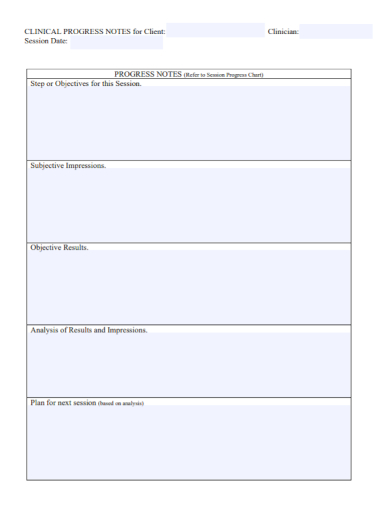
6. Clinical Progress SOAP Note
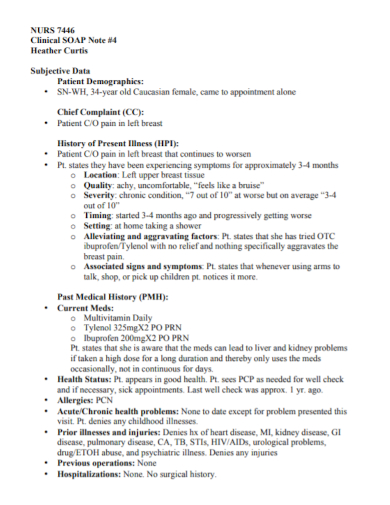
7. Clinical Nurse SOAP Note
8. Clinical SOAP Report Note
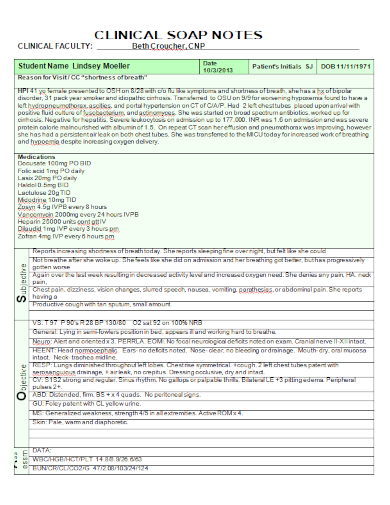
9. Clinical Faculty SOAP Note
10. Clinical Nutrition SOAP Note
What is a Clinical SOAP Note?
Also known as a client progress note or DAP (Data, Assessment and Plan), a SOAP (Subjective, Objective, Assessment and Plan) note demonstrates a short and explicit medical overview of each therapy or treatment session of the patient and a all-inclusive record of the therapy or treatment plan to the patient.
In addition, it is an essential document that presents solid goals and objectives, as well as the whole development or overall progression of your patient’s physical therapy, rehabilitation for mental health due to drug and alcohol abuse, accidents, trauma, or any other incidents.
How to Write a Clinical SOAP Note
While you are doing your best effort on facilitating several types of treatments for your patients, you also need to be able to write a clear and in-depth clinical SOAP note or progress report of your clients to evaluate and closely monitor their individual progress and show feedback to the clients’ guardians or parents about the progress in their therapy or treatment plan.
In this section, we give you some easy-to-follow tips that indicate how to design a well-detailed clinical SOAP note for your patients:
1. Keep up a good and amicable relationship with the patient
By using some constructive yet empathetic questions to ascertain and bring out your patient’s real thoughts, and feelings, you can understand the condition of your patient. Most significantly, you need to think about keeping up a good and amicable relationship with your patient to encourage change and more progress. Constantly review your methods.
Continue on performing your best effort when you show warmth and friendliness to your client during the therapy. Make eye contact and allow time for small talk. Then, ask your client about his or her problem.
2. Create assessment of your patient’s needs
After your patient opens up, you can now create some assessment of your patient’s needs. Research about the diagnosis you made according to his or her physical, emotional, and mental condition.
Take notice of the methods and prescriptions that are crucial for your patient’s therapy or treatment plan. Incorporate all of this information to the SOAP note as this will be the outset stage of his or her progress of the medical treatment.
3. Interpret the outcome of the therapy
Then, after several weeks of the therapy, interpret the outcome of the therapy in detail. Observe the new symptoms that he or she is currently feeling due to the intake of some medications. Use some charts, graphs, tables and other visual diagrams while you make some medical interpretations of the patient’s condition after taking the treatment.
Conduct some careful observations of your patient for another week or even months, depending on his or her medical condition. Record every little detail of your patient’s progress in your clinical SOAP note. Ask the patient’s parents or guardians about his or her condition at home, at school, etc.
4. Use some psychological evaluation tests
Psychological evaluation tests or assessments are integral tests that you should conduct so that you are able to measure and keep track on the progress of your patient. This series of tests is a valuable tool in gathering sufficient information about how your clients think, feel, behave, and react. The findings are used as references to develop a medical report or a clinical SOAP note of your patient’s abilities and behaviors, and providing necessary recommendations for his or her treatment.
FAQs
When writing an effective clinical SOAP note, you need to look for the proper time in recording the progress of the client’s treatment session, keep using a professional tone, don’t use complex or complicated terms and phrases, avoid the use of negative phrasing, maintain your notes clear and brief, avoid confusing pronouns, and continue writing with accuracy without judgment. [/ns_row ]
A SOAP note contains the subjective, objective, assessment, and plan. It gives a well-detailed documentation of the chart of a patient along with the admission note. How to write a SOAP note?
What are the four parts of a SOAP note?
In writing a SOAP or progress note for therapy, use clear and brief terms and phrases. Focus on the appropriate spelling, right point-of-view or person perspective, and proper tense. Make your notes short and straightforward. How to write a SOAP note therapy?
A client’s psychological health records which include the SOAP notes must be kept by all licensed psychologists or mental health therapists for a minimum of seven years from the discharge date of the patient or seven years after a minor patient becomes 18 years old. How long do I need to keep SOAP notes?
Therefore, writing an all-inclusive clinical SOAP note for your client is a crucial method in promoting good communication between physicians, pharmacists, therapists, social workers, and other medical professionals in facilitating the teaching or learning method. Being extensively used by a variety of medical and rehabilitation professionals, clinical SOAP notes focus exclusively on the patient’s clinical problem rather than creating a summary of the diagnosis. Additionally, these notes reiterate adherence to a documentation style to prevent possible misinterpretation. Here are some of our downloadable and printable clinical SOAP note samples available in different kinds of formats.
Related Posts
FREE 21+ Delivery Note Templates
FREE 17+ Sample Doctors Note
FREE 15+ SOAP Note Templates
FREE 12+ Medical Officer Job Description Samples
FREE 11+ Sample Doctors Note
FREE 9+ Sample SOAP Note
FREE 9+ Sample Clinic Note
FREE 9+ Statistical Analysis Plan Templates
FREE 8+ Nursing Note Templates
FREE 8+ Sample Soap Note
FREE 13+ Sample Discharge Summary
FREE 12+ Medical Records Request Forms
FREE 12+ Sample Mood Chart
FREE 10+ Patient Case Study Samples
FREE 10+ Sample Quality Assurance Job Description