
Whenever a working individual falls ill and has to file a leave of absence from work, there are company leave rules that need to be followed, which means the individual just cannot take time off from work without a valid reason. That is why a medical certificate presents a bona fide proof that the individual has been sick and had gotten medical help from a health-care provider.You may also see medical certification forms
Our sample certificates for medical forms from health-care providers present users with a guide on how medical certificate formats are being formulated. These are all free for downloading in both Word Doc and PDF file formats.
Download Medical Certificate Forms Bundle
FMLA Medical Certification Form
FMLA Medical Certification Form
Employee Information
- Name: [_______________]
- Job Title: [_______________]
- Department: [_______________]
- Contact Number: [_______________]
Medical Condition
- Description of the condition requiring leave: [_________________________________]
- Date condition commenced: [_______________]
- Estimated duration of condition: [_______________]
Care Requirements
- Does the patient require inpatient care?
- Yes
- No
- Does the patient require continuing treatment by a health care provider?
- Yes
- No
Treatment Schedule
- Frequency of treatment: [_______________]
- Duration of treatment: [_______________]
- Dates of scheduled treatment, if applicable: [_______________]
Health Care Provider Information
- Name: [_______________]
- Address: [_______________]
- Phone Number: [_______________]
- Type of Practice/Specialization: [_______________]
Certification
- I certify that the information provided is accurate to the best of my knowledge and that the employee requires FMLA leave for the reasons stated above.
- Signature of Health Care Provider: [_______________]
- Date: [_______________]
Employee Signature
- I understand that the information provided will be used for the purpose of validating my FMLA leave.
- Signature of Employee: [_______________]
- Date: [_______________]
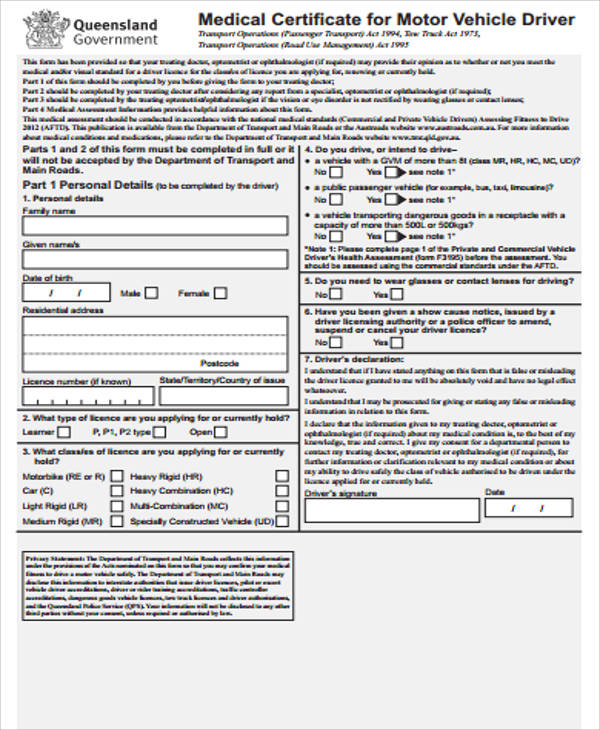
CDL Medical Certificate Form
Section 1: Driver Information
- Name (Last, First, Middle): ___________________________________
- Date of Birth: _______________
- Driver’s License Number: ___________________
- Phone Number: ___________________
- Address (City, State, Zip): ___________________________________
- Email Address: ___________________
Section 2: Health History
- Questions about the driver’s medical history, including conditions like heart disease, high blood pressure, epilepsy, diabetes, and any history of alcohol or drug abuse. Drivers must answer “Yes” or “No” to each condition and provide details if the answer is “Yes.”
Section 3: Vision Test
- Right Eye: ___________
- Left Eye: ___________
- Both Eyes: ___________
- Corrective lenses required? (Yes/No): _______
Section 4: Hearing Test
- Hearing ability in the better ear (with or without hearing aid): ___________
Section 5: Blood Pressure/Pulse Rate
- Blood Pressure: ___________
- Pulse Rate: ___________
- Indicates cardiovascular health and potential for hypertension.
Section 6: Laboratory and Other Test Findings
- Includes results for urine analysis and may require additional testing based on medical history and examiner’s findings.
Section 7: Medical Examiner’s Certification
- The medical examiner must certify that based on the examination, the driver:
- Meets the physical qualification requirements of the CDL without any restrictions.
- Meets the physical qualification requirements with certain restrictions (to be listed).
- Does not meet the physical qualification requirements.
- Medical Examiner’s Name: _________________________
- Signature: _________________________
- Date: _______________
- License Number: _______________
- Phone Number: ___________________
Additional Notes
- Space for the examiner to provide any additional observations or recommendations.
Medical Certificate Forms Online
Patient Information:
- Name: ____________________________________
- Date of Birth: _____________________________
- Address: __________________________________
- Phone Number: ____________________________
Examination Date:
- Date: ____________________________________
Medical Examination Details:
- Height: ___________
- Weight: ___________
- Blood Pressure: ___________ / ___________
- Pulse Rate: ___________ beats per minute
- Temperature: ___________ °F/°C
Medical History Review:
- Any known allergies: _______________________
- Current medications: _______________________
- Past surgeries or hospitalizations: ____________
- Chronic illnesses (e.g., diabetes, hypertension): ________________
Physical Examination Summary:
- General Appearance: [Healthy/Frail/etc.]
- Eyes: [Normal/Abnormal – specify if necessary]
- Ears, Nose, Throat: [Normal/Abnormal – specify if necessary]
- Cardiovascular System: [Normal/Abnormal – specify if necessary]
- Respiratory System: [Normal/Abnormal – specify if necessary]
- Gastrointestinal System: [Normal/Abnormal – specify if necessary]
- Musculoskeletal System: [Normal/Abnormal – specify if necessary]
- Neurological System: [Normal/Abnormal – specify if necessary]
- Dermatological Condition: [Normal/Abnormal – specify if necessary]
Physician’s Findings and Recommendations:
- [Details of findings, diagnosis, and any recommended treatments or follow-up actions.]
Certification:
- I certify that I have examined the above-named patient and, to the best of my knowledge, he/she is in [state of health, e.g., good/poor] health.
Physician’s Signature and Stamp:
- Signature: _________________________________
- Name: ____________________________________
- Qualification: _____________________________
- Registration Number: _______________________
- Date: ____________________________________
- Stamp: ___________________________________
Medical Certificate Forms For Leave
Patient Information
- Name: __________________________________________________
- Date of Birth: ______________________
- Employee ID (if applicable): ______________________
- Department: ______________________
- Position: ______________________
- Contact Number: ______________________
Medical Condition
- Diagnosis: __________________________________________________
- Description of Illness/Injury:
- Date of Onset: ______________________
- Date of Medical Consultation: ______________________
- Expected Duration of Absence:
From ______________________ To ______________________
Treatment Plan
- Medications Prescribed:
- Required Rest/Recovery Period:
- Follow-up Appointment Date: ______________________
Physician’s Information
- Name: __________________________________________________
- Qualification/Specialization: ______________________
- Medical License Number: ______________________
- Contact Number: ______________________
- Signature: ______________________
- Date: ______________________
Employer Certification
- Received by (Name & Title): ______________________
- Date of Receipt: ______________________
- Signature: ______________________
Employee Acknowledgment
- I acknowledge that the information provided is accurate to the best of my knowledge and will be used to assess my leave request.
- Signature: ______________________
- Date: ______________________
Browse More Templates On Medical Certificate Forms
Medical Certificate PDF Free Download
Medical Certificate Sample PDF
What Documents Need For Medical Certificate?
When obtaining a medical certificate, the specific documents required can vary depending on the country, the purpose of the certificate, and the healthcare provider’s policies. However, commonly required documents include:
- Identification: Valid government-issued ID (passport, driver’s license, or national ID card) to verify your identity.
- Medical History Forms: You might be asked to fill out forms detailing your medical history to assist the healthcare provider in making an accurate assessment.
- Previous Medical Records: Any relevant medical records, test results, or letters from other doctors that relate to the condition for which you’re seeking a medical certificate.
- Proof of Appointment: Confirmation of your appointment with the healthcare provider, if required.
- Payment Information: Insurance details or payment method for the consultation and issuance of the certificate.
- Specific Documentation: For certain types of medical certificates, such as those needed for work, school, or travel, you may need to provide specific forms or documents for the doctor to complete or reference.
Always check with the issuing authority (e.g., your employer, school, or consulate) for their specific requirements and with the healthcare provider for any additional documentation they may need.
Medical Certificate Form
Medical certificate forms can be used not just by company employees but almost all individuals who need to have medical clearance like students and drivers who need them to assure the organization he’s working for that he’s fit to drive. Our sample forms are taken from generic sample forms or used with permission from medical clinics that issue standard forms for medical certificates.You may also see medical clearance form
For students meanwhile, each school has a different guideline on the issuance of medical certificates for students who have missed a couple of school days. Some schools print their own standard medical certificate forms that are being issued to sick students who need to fill out and submit them to their doctor. Instead of making one or using the medical institution’s form, all the doctor needs to do is to fill out the school form and sign on all the necessary spaces.You may also see return to work medical form
Since each school has different guidelines for medical certificates, it’s important that students need to check their own school guidelines for medical certificates before using our samples. There are also schools that require students to file sick leave and also attach a medical certificate to it.You may also see medical certificate from doctor
Sick Leave Medical Certificate Form
How to Fill Out a Medical Certificate Form
Filling out a medical certificate form accurately is crucial to ensure it serves its intended purpose, whether for sick leave, fitness assessments, or other medical needs. Here’s a general guide on how to complete one:
- Personal Information: Start by providing your full name, date of birth, address, and any other personal identification details required on the form. Ensure this information matches your official ID documents.
- Date of Visit: Enter the date you visited the healthcare provider for the assessment related to this certificate.
- Medical Professional’s Details: The form may require the name, address, and contact information of the medical professional or institution issuing the certificate. This section is often filled out by the healthcare provider.
- Diagnosis or Reason for Visit: Include the medical reason for your visit. This could be a diagnosis, symptoms, or the purpose of the medical examination. Note that the level of detail required here can vary based on privacy laws and the intended use of the certificate. In some cases, the healthcare provider may choose to keep this section vague to protect patient privacy.
- Period of Absence: If the certificate is for sick leave, specify the dates you are excused from work or school. This includes the start date and the anticipated return date.
- Limitations or Recommendations: If applicable, detail any specific limitations or recommendations from the healthcare provider. This could include restrictions on certain activities or advice for phased return to work or school.
- Healthcare Provider’s Declaration: This section is typically reserved for the doctor or medical professional to fill out. It may include their assessment, any pertinent medical information they can disclose, their signature, and the date of signing.
- Patient or Guardian Signature: If required, sign the form to acknowledge the accuracy of the information provided. If the patient is a minor or unable to sign for themselves, a guardian may need to sign.
- Additional Documentation: Attach any additional documentation required by the entity requesting the medical certificate. This might include identification documents or previously issued medical reports.
Before submitting the form, double-check all entries for accuracy and completeness. Remember, the requirements for medical certificates can vary widely, so it’s essential to follow any specific instructions provided by the entity requesting the certificate or by the healthcare provider issuing it.
Medical Certificate Sample
Medical Certificate Form PDF For Students

For students who miss important term exams, the allowable time to apply for special examination is usually within five working days from the date of the missed examination. Some even shorten the application time to three days even with accompanying medical certificates. Schools are quite strict about their students adhering to guidelines, so when a student fails to file an application for a makeup exam during the standard allowable time, he or she may not be allowed to take the exams even when submitting a medical certificate. You may also see medical certificate for school
For other medical-related job description samples, please check on our Medical Examiner Job Description examples for states or counties who need medical examiners for their own investigative agencies. These samples are all free for downloading in both Word Doc and PDF files.
Tips For Filling a Medical Certificate Form
Filling out a medical certificate form accurately is essential, as it’s a legal document that can impact your employment, insurance claims, or academic considerations. Here are some tips to ensure you complete the form correctly:
- Read Instructions Carefully: Before starting, read all instructions on the form. Understanding what’s required will help you fill it out correctly and avoid mistakes.
- Use Legible Handwriting: If the form must be filled out by hand, write clearly and legibly. Unclear handwriting can lead to misunderstandings or processing delays.
- Provide Accurate Information: Ensure all information is accurate and truthful. Misrepresenting your health condition can have legal or disciplinary consequences.
- Double-Check Personal Details: Verify your personal information (name, date of birth, address) matches your identification documents. Discrepancies can cause delays or rejection of the form.
- Be Concise but Thorough in Descriptions: If you’re required to describe symptoms or reasons for the visit, be concise but provide enough detail to explain your situation clearly.
- Understand Privacy Implications: Be aware of what medical information you are sharing and with whom. If you’re concerned about privacy, discuss with your healthcare provider what details need to be disclosed.
- Know the Period of Validity: Clearly indicate the relevant dates, especially if the certificate relates to a period of absence from work or school. Include both the start and expected end dates.
- Consult Your Healthcare Provider: If unsure about any section, ask your healthcare provider for clarification. They can provide valuable advice on how to correctly fill out the form.
- Attach Additional Documents if Required: Some medical certificates require supporting documentation. Attach any additional sample reports or letters from specialists if needed.
- Review Before Submission: Before submitting the form, review all sections to ensure completeness and accuracy. Missing or incorrect information can lead to unnecessary delays.
- Keep a Copy: Always keep a copy of the completed form and any other submitted documents for your records.
- Submit Promptly: Ensure the form is submitted within any required deadlines, especially if it’s related to work leave, insurance claims, or academic accommodations.
Following these tips will help ensure your medical certificate form is filled out accurately and efficiently, facilitating smoother processing for whatever purpose it serves.
Download Medical Certificate Form
Medical Certificate Application Form
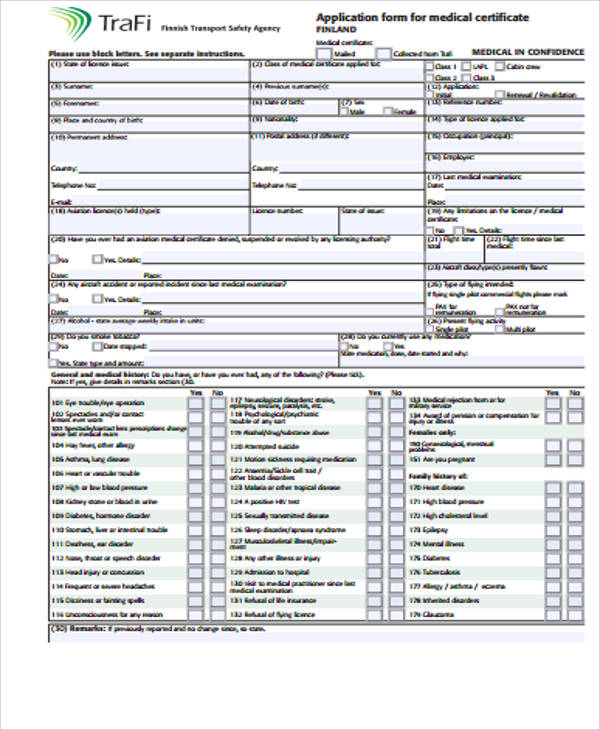
The format for medical certificates form often describes the diagnosis for the illness and the treatment being administered by the attending physician. The forms help describe the treatment process, what medicines were being administered, and the days when the patient needed to be confined or advised for a bed rest.You may also see medical fitness certificates
Besides serving its purpose as an explanation for being absent for work or needing bed rest and time away from work, a medical certificate may be used for a variety of reasons such as obtaining health benefits from the company or making an insurance claim.You may also see printable medical forms
For more examples of Medical Certification Forms, please click on the link which will guide you to a couple more examples of standard medical certification forms that you can use to have your health-care provider use them to fill out your certification.
What is a medical certificate letter?
A medical certificate letter is a document issued by a healthcare professional to confirm a person’s medical condition, diagnosis, treatment, or ability to perform certain activities, often needed for work or legal purposes.
What is a medical certification requirement?
Medical certification requirements refer to the necessity of providing a medical certificate or documentation to meet specific standards or fulfill obligations, often in contexts such as employment or legal matters.
How to confirm that the Medical Certificate is on my driving record
To confirm if a Medical Certificate is on your driving record, contact your local DMV or relevant authority, or check your driving record online through their official website or request a copy.
In conclusion, these medical certificate forms serve as vital documentation, providing accurate records of an individual’s health status. Completing these sample forms thoroughly ensures comprehensive and reliable information for medical assessment. We appreciate your diligence in maintaining up-to-date medical records, contributing to the well-being and safety of our community.
Related Posts
FREE 9+ Sample Attractive Photography Gift Certificate Templates in PSD | MS Word
FREE 36+ Sample Certificate of Completion Templates in AI | InDesign | MS Word | Pages | PSD | Publisher | PDF
FREE 8+ Divorce Certificate Samples in MS Word | PSD | AI | Publisher | Pages | InDesign | PDF
FREE 11+ Sample Performance Certificate Templates in PDF | MS Word | AI
FREE 4+ Certification of No Record Samples in PDF | MS Word
FREE 10+ Yoga Certificate Samples in MS Word | PSD | AI | Publisher | Pages | Indesign | Google Docs | PDF
FREE 7+ Sample Birthday Gift Certificate Templates in EPS
FREE 10+ Company Incorporation Certificate Samples in Google Docs | Pages | MS Word | PDF
FREE 10+ Salon Gift Certificate Samples in MS Word | PSD | AI | Publisher | Pages | Indesign | Google Docs | PDF
FREE 10+ Pet Birth Certificate Samples in MS Word | PSD | AI | Publisher | Pages | Indesign | Google Docs | PDF
FREE 11+ Wedding Certificate Templates in PDF | MS Word | PSD
FREE 6+ Sample Thank You Certificate Templates in PDF | MS Word | PSD
FREE 17+ Soccer Certificate Templates in PSD | AI | InDesign | MS Word
FREE 25+ Sample Participation Certificates in AI | InDesign | MS Word | Pages | PSD | Publisher | PDF
FREE 60+ Sample Gift Certificate Templates in PDF | PSD | MS Word | AI